What does the placenta look like and where is it attached?

The placenta is the only organ in the body of a woman that performs essential functions, but at the same time is temporary. In the process of carrying a baby can not do without him, but after the birth of a child in it there is no need. Much depends on the structure of the placenta and its location during pregnancy: the characteristics of gestation, the mode of delivery. How the placenta attaches to the female body, and what it affects, we will explain in this article.

Structure and functions
If you translate the Latin word placenta, you get the "cake". This is what this body looks like. In the people it is called "children's place". The placenta does not begin to form immediately after conception of the baby, but only after 8-10 days, when the fertilized egg falls into the uterus and attaches to its inner wall using chorionic villi (part of the fetal membrane).
From this point on, the chorion - the precursor of the placenta - is responsible for feeding the embryo, supplying it with oxygen and producing the hormones necessary for carrying the fetus. The placenta itself forms gradually and begins to act from about 13-14 weeks of pregnancy. The “baby seat” grows until the middle of the second trimester, then its growth stops, and the placenta begins to gradually “fade out”, “grow old”. For childbirth, it completely exhausts its resource and is born 15-60 minutes after the birth of the baby.

The structure of the placenta is quite complex, and each of its layers provides its own functions. In general, it is a spongy organ densely saturated with a network of blood vessels communicating with lacunae filled with maternal blood. The value of the placenta for a growing baby is difficult to overestimate - it protects the child, creating a hemoplacental barrier.
The “baby seat” passes to the baby in the womb the antibodies produced by the mother’s immunity, which provides the child with innate passive immunity. Some not the most useful substances that enter the mother's body are blocked and retained by one of the layers of the placenta, not passing them to the baby.
The placenta feeds the child, performing the functions of gas exchange. From my mother's blood through the "baby place" oxygen enters the baby, carbon dioxide is removed back. By giving the child access to vitamins and minerals, as well as water, the placenta brings the products of the metabolism of crumbs - urea, creatine and creatinine back to the mother's body.

During pregnancy, the “baby seat” is also the endocrine gland - it produces some of the hormones necessary for the preservation of pregnancy and the development of the fetus. First of all, it is hCG, produced immediately after implantation with chorionic villi, as well as placental lactogen, which is necessary for the preparation of the mammary glands for the upcoming breastfeeding. The placenta produces prolactin, which is responsible for the lactation process, progesterone, which is responsible for the safety of pregnancy and the prevention of menstruation, as well as serotonin, estrogen and relaxin.
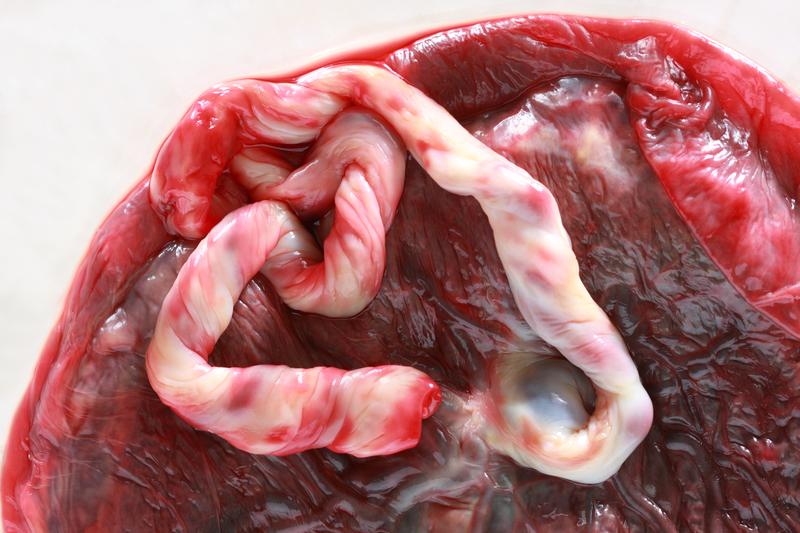
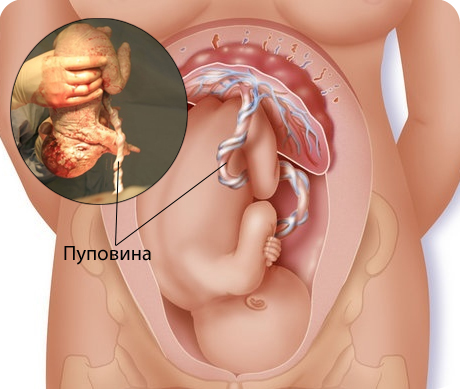
The placenta is conventionally divided into two parts - the fetus, which is on the child’s side, and the maternal part, adjacent to the wall of the uterus.From the fruit side, the umbilical cord is attached to the central part of the placenta - a strong cord that connects the fetus itself and the “children's place”.

Types of location
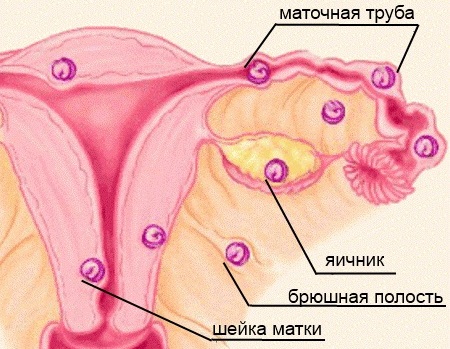
The placenta in the uterus is formed where the fertilized egg was able to consolidate at the time of implantation. Much of this delicate process depends on the state of health of the woman, on the state of the endometrium, hormonal levels, the general state of the reproductive system of the future mother, as well as on the correctness of the formation of the ovum.
Optimal and correct is the attachment of the chorion (and later the placenta) on the front or back wall of the uterus closer to its bottom. The bottom is not at the bottom, as it may seem, at first glance, but at the very top of the uterus.
The farther away from the exit into the vagina the “baby seat” is located, the better the pregnancy will proceed and the more optimistic the predictions for the upcoming delivery.

If a woman has endometriosis, fibroids, there are abnormalities in the structure of the uterus, if she has performed abortions before, has postoperative scars on the uterus, then it is quite possible that the fertilized egg will not be able to consolidate in a suitable place and will fall below. Then the attachment will be low and may subsequently cause pathologies such as placenta previa, its regional attachment.
Some experts argue that the place of attachment of the ovum affects not only the health of the expectant mother, the presence of bad habits and fetal factors, but also gravity. The essence of the theory is that the fetus is more likely to entrench where it is more likely to be - if a woman prefers to sleep on the left side, then the fetal egg will be located on the left side of the uterus. However, convincing scientific evidence of this theory does not yet exist.
However, it is absolutely certain that the fruit will never be fixed where it is unsafe and inconvenient to develop and grow. If there are tumors in the uterus, scars, the fertilized egg with amazing accuracy will pass them and find another place for itself, perhaps not always normal, from the point of view of doctors, because of the danger of complications during gestation and during childbirth.

With the normal location of the placenta, the growing uterus creates the most favorable conditions for the development of the baby - the edges of the placenta move to the side of the uterus as they grow, and the blood supply becomes more intense, sufficient and satisfying all the needs of the tiny organism.
Placenta previa, in which the “baby seat” is at the bottom, completely or partially blocking the exit to the pelvis, is a serious and dangerous pathology that threatens miscarriage, premature birth, and the development of severe bleeding in the event of spontaneous detachment, which can cause the death of the mother and fetus. The marginal attachment is less dangerous, but also pathological.
The lower location of the placenta, in which it does not affect the entrance to the cervical canal of the cervix and does not block the exit to the small pelvis, although it is considered pathological, has more favorable projections. The growing uterus stimulates the rise (migration) of the placenta above, which occurs in the vast majority of cases.

Let us consider in more detail some of the most common types of location of the “children's place”
On the front wall
On the anterior wall of the uterus, the fertilized egg is usually attached to women who have already had time to bear and give birth to babies. Primiparous women are less likely to face placentation on the front wall. In itself, this arrangement is considered a variant of the norm and does not need treatment. Low anterior location is a risk factor in terms of the likelihood of placental abruption, but such an arrangement of the “baby seat” is rarely observed.
If the placenta is located on the front wall, the woman usually feels the fetal movements later than the others; the movements themselves are not as strong and pronounced.But this fact, of course, will please the future mother in the later stages of gestation, when there is little free space in the uterus, and the babies begin to kick painfully.

On the back wall
On the back wall "baby seat" is located most often. This is a classic standard. The posterior wall of the uterus in its upper part (closer to the bottom) is best supplied with blood. The placenta, located behind, does not prevent a woman from early to feel the first movements of her baby. In addition, the placenta located on the back wall is more difficult to injure in the fall or blunt injury.

Low location
Low attachment is indicated if the edge of the placenta is only 6 centimeters higher than the internal osma of the uterus. If the baby is too active, it can damage the "baby seat", the weight of the fetus, which grows, will also be a risk factor for premature detachment of the placenta.
Low placentation poses a threat to the development of hypoxia if partial detachment occurs and can also prevent natural childbirth. Women in whom the placenta does not rise as the duration of pregnancy increases (about 3%) do not migrate, usually give birth through surgery, they are given a cesarean section.

Previa
If the edge of the placenta closes the inner pharynx by about a third, they say about partial or incomplete presentation, if the “children's place” covers it completely, this dense, total presentation is an unconditional and undoubted indication for a cesarean section.
This complication threatens the occurrence of bleeding during childbearing, and is also dangerous in the event of spontaneous labor, the occurrence of massive bleeding, the development of acute hypoxia in the baby, his death, as well as the death of the mother as a result of blood loss.

Incremental (optional) lobe of the placenta
This pathology is found in about 8% of pregnant women. The placenta with an additional lobule consists of a large body and a small one, which are connected by blood vessels and a membrane. The umbilical cord is always attached to a large lobe. During the carrying of the child, the additional slice does not represent a special danger, but at birth she risks loosening up, causing bleeding.
Obstetricians, taking urgent delivery, do not always know for sure about the presence of an additional lobe, and it may well remain in the uterus after delivery. This situation will require additional curettage, as the woman will develop a strong inflammatory process.
In the early stages, an additional share is not visible to anyone, because the form of the placenta takes on only by the fourth month.


It is important to establish an appropriate diagnosis before delivery, so that the postpartum complications do not arise.
Is it possible to affect the attachment of the placenta?
Neither the woman herself, nor the best and most experienced doctors are able to influence where the fertilized egg is finally attached, and where the formation of the placenta will begin. But a woman can take care of the normal course of her pregnancy in advance, warning risk factors for the wrong arrangement of the “baby seat”.
First of all it concerns the observance of intimate hygiene and visiting a doctor. Constant sexual partner and careful attention to their health will help to avoid infections and sexually transmitted diseases, which at times increase the likelihood of previa or a low location of the placenta.
Bad habits (smoking and alcohol) should be abandoned at the planning stage of the baby. All diseases of the gynecological profile should be thoroughly examined and treated to the end, since the chronic "female sores" can affect the condition of the endometrium of the uterus and play a negative role in the implantation of the ovum.


Abortions and scraping do not pass without a trace for the state of the inner lining of the female reproductive organ. They are best avoided.
It is important to plan the second, third, fourth and subsequent pregnancies after examination by a doctor, because with each subsequent pregnancy the probability of an abnormal location of the placenta increases. If in previous pregnancies the placenta was inferior or presumed, the consultation of the doctor is obligatory - quite often there is a relapse of such phenomena.
Taking medications that have not been prescribed or approved by a doctor, especially antibiotics, hormonal drugs, hemostatics before conception or a month before conception planning, can also affect not only the location of the placenta, but also its structural features.

In order to avoid problems with the placentation after conceiving a long-awaited baby, a woman does not need to experience serious physical overloads, lift weights, special attention should be paid to the preliminary treatment and correction of diseases such as diabetes and thyroid diseases.
The fact that such a placenta, see the following video.









