Third cesarean section: features and opinions of doctors

Caesarean section in the old days was considered an operation of despair. He was made when it was no longer possible to save a woman, only to try to save the child. Modern medicine has in its arsenal new technologies for the operation, a qualitatively new suture material, as well as antibiotics, and therefore the Cesarean section is practiced more often, and the list of indications for it is increasing. In all cases, when natural childbirth can be dangerous for the child and his mother, a cesarean section is performed. And this is not a sentence, because after the first such operation, a woman can become a mother and the second, and the third, and even subsequent times.
In this article we will talk about what constitutes the third cesarean section, the risks it is associated with and how the operation goes.

Hazards and Risks
If a woman already has two children, and both were born by caesarean section, a third pregnancy will always be considered risky. The whole thing - in the presence of a scar on the uterus. During gestation of the fetus, the female reproductive organ grows, stretches, a total of the uterus grows 500 times compared with the size before pregnancy.
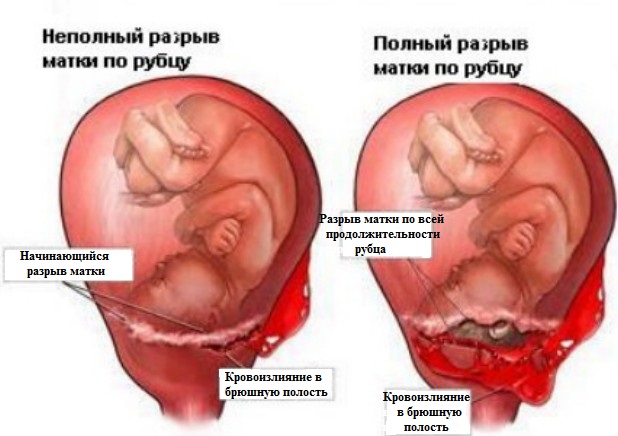
Connective tissue dominates in the scar area. It is no different elasticity, and therefore worse to stretch. The third pregnancy, therefore, automatically “records” a woman after the first two at risk for the likelihood of pregnancy complications, the most formidable of which is rupture of the scar. The gap could theoretically occur at any time, and this is precisely what the doctors of antenatal clinics are most afraid of., because in most cases the rupture of the scar is lethal for the baby and his mother.

In addition, a scar on the uterus increases the likelihood of low placentation, placental insufficiency, placental abruption, intrauterine growth retardation.
That is why in the eyes of an obstetrician-gynecologist in consultation there is no great joy and enthusiasm when a woman comes to him to register for pregnancy, who is to undergo a third cesarean section. This is understandable - no one doctor needs corrupted statistics. The question of the danger of a third pregnancy is largely exaggerated.
And often the doctors themselves are exaggerating it, and they will be responsible for the future mother and possible complications.
In practice, the rupture of the scar with the onset of labor activity occurs in about 5–9% of cases, and during pregnancy this probability is less than 1%. Nevertheless, there are risks, and you need to know about them.

Pregnancy may occur after a short period of time after a previous operation (if 2 years have not passed, it is better to abstain from pregnancy).
Not too good and the break between the birth more than 5 years. The older the scar becomes, the less elastic it is. The initial thickness of the scar before pregnancy is also important (it should not be less than 7 mm). The scar should be uniform, without "niches".


From a woman in the process of carrying a third pregnancy will require discipline. She will have to come to the doctor more often than other pregnant women, she will be more likely to do an ultrasound scan, including in order to examine the scarring zone during the growth of the uterus.
From the end of the second trimester, it is recommended to do an ultrasound scan 2 times a month, and in the third trimester - once every 10 days.
Much depends on the state of health of the pregnant woman, on her age, on the place of attachment of the placenta. Tactics of conducting such a pregnancy is determined individually. Only one question is not discussed - about delivery. Natural childbirth after two operations of the COP can not be. It is deadly for women and children. Delivery is always done surgically.

How is the third operation?
The operation is carried out as planned. The woman can choose the date herself, provided that the doctor agrees with the choice.
Usually, the third cesarean section is carried out for a period of 38-39 weeks in order to exclude the likelihood of self-delivery due to the risk of rupture of the uterus along the scar during labor. Operate and 36-37 weeks, if the doctor has reason to suspect that a woman can begin childbirth. But before the expected date of birth (PDR) don’t give a pregnancy.
The operation, like the previous two, is performed using anesthesia.
Most of these genera are now taken with epidural (spinal) anesthesia. It gives the opportunity to "participate" in the process, to see the child immediately after his birth.
Also, a woman may refuse to inject an anesthetic drug into the spinal canal and ask for general anesthesia, in which she will be “absent” at her own birth, and will meet with the child only after a few hours.


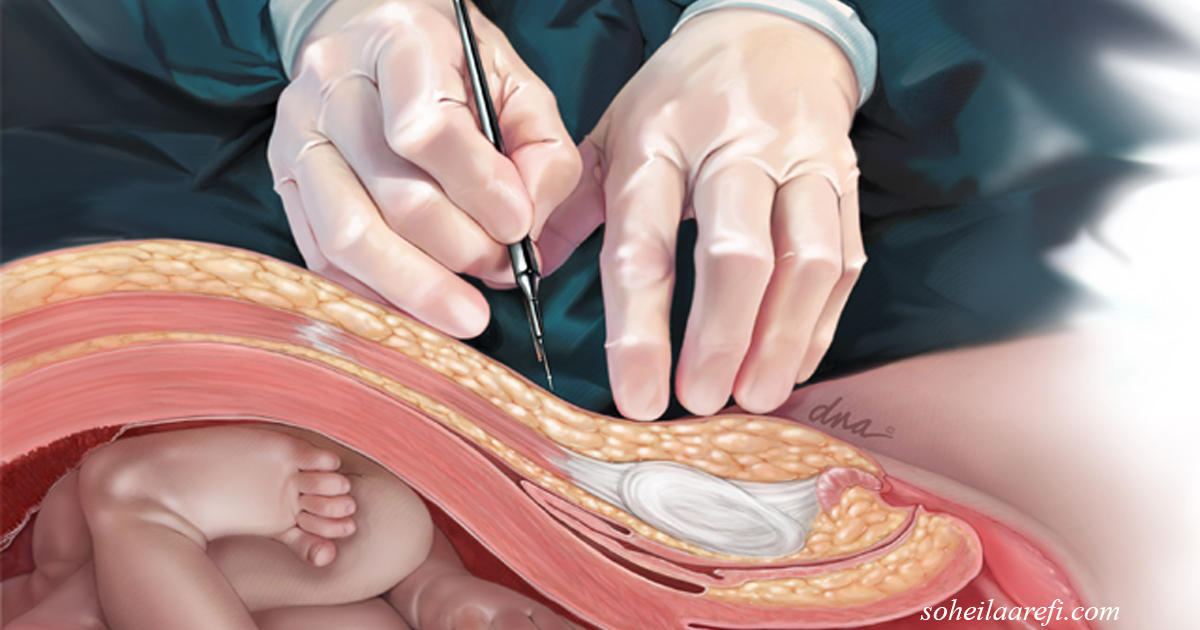
The operation is performed on the old scar, which means that the doctor makes an incision where there was a dissection during the previous operation. The spikes and the old scar are excised.
The incision today is done horizontal in the lower uterine segment. At this point, the tissue is scarring better, healing is faster, and the lower segment of the reproductive organ is less stretched during subsequent pregnancy (if the woman wants a fourth child).
After an incision, the muscles are separated to the sides, and the bladder is also withdrawn to the side. Then make an incision on the uterus, pierce the fetal bladder. The child is removed, cut off the umbilical cord. The baby is transferred for processing and weighing, and the surgeon manually separates the placenta.

After that, the uterus is sutured, restore the position of the muscles of the peritoneum, impose external sutures.
The operation usually lasts about half an hour. But in the case of the third in a row, the duration of surgical intervention may be somewhat longer, because additional time is required for excision of the old connective tissue.
After surgery, 24-hour close observation of the woman is recommended during the day. A woman must always be given contraction medications so that the uterus is better contracted. Sometimes antibiotics are indicated. Almost always recommended painkillers within 1-2 days after surgery. It is believed that the earlier the child is applied to the breast, the better and faster the uterus will contract, the less postoperative complications may be.
A woman can get up in a day. Long lying in bed is not welcome.

How to prepare?
Preparation should begin at the planning stage of pregnancy. Many difficulties both in carrying a child and during an operation can be avoided if the risks are maximally calculated in advance. To do this, you need to be protected after the previous cesarean section and to exclude the possibility of abortion, scraping, operations on the uterus.
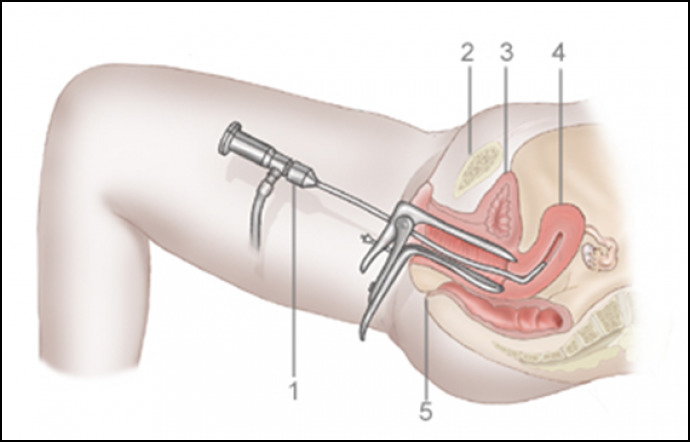
After a two-year break, be sure to visit a gynecologist. It is recommended to make not only ultrasound scans with the assessment of the state of the scar (outside of pregnancy is not very informative), but also hysteroscopy and hysterography with contrast. These diagnostic studies allow us to identify the viability of scar tissue, its homogeneity, possible notches and thinning areas.
Reviews of patients and doctors
According to women, the third cesarean section passed, like the previous ones, the subjective sensations differed little. The period after the operation, according to the mothers, was a little faster than the previous times, because I already had the skill and understanding how to change the position of the body after the operation, how to sit down, stand up, take steps. There was no fear of an upright posture after the operation.
The opinion of doctors in recent years has become more supportive, but they continue to insist on a preliminary thorough examination of the scar. If the scar tissue has a thickness of less than 2.5 mm, if there are heterogeneous fragments, thinning, then the woman is recommended to abandon plans to become a mother for the third time.

Reviews of women show that the efforts of doctors and the possibilities of modern medicine make it possible to carry a child with a thin scar, and with niches for scar tissue, but finding a clinic that would undertake to conduct such a pregnancy is very, very difficult.
Doctors and clinics that specialize in this, not so much. But they are there, which means that there is a chance for motherhood for the third time even for those whose scars were recognized insolvent in consultation at the place of residence.

On the consistency of scars on the uterus experts tell in the next video.









